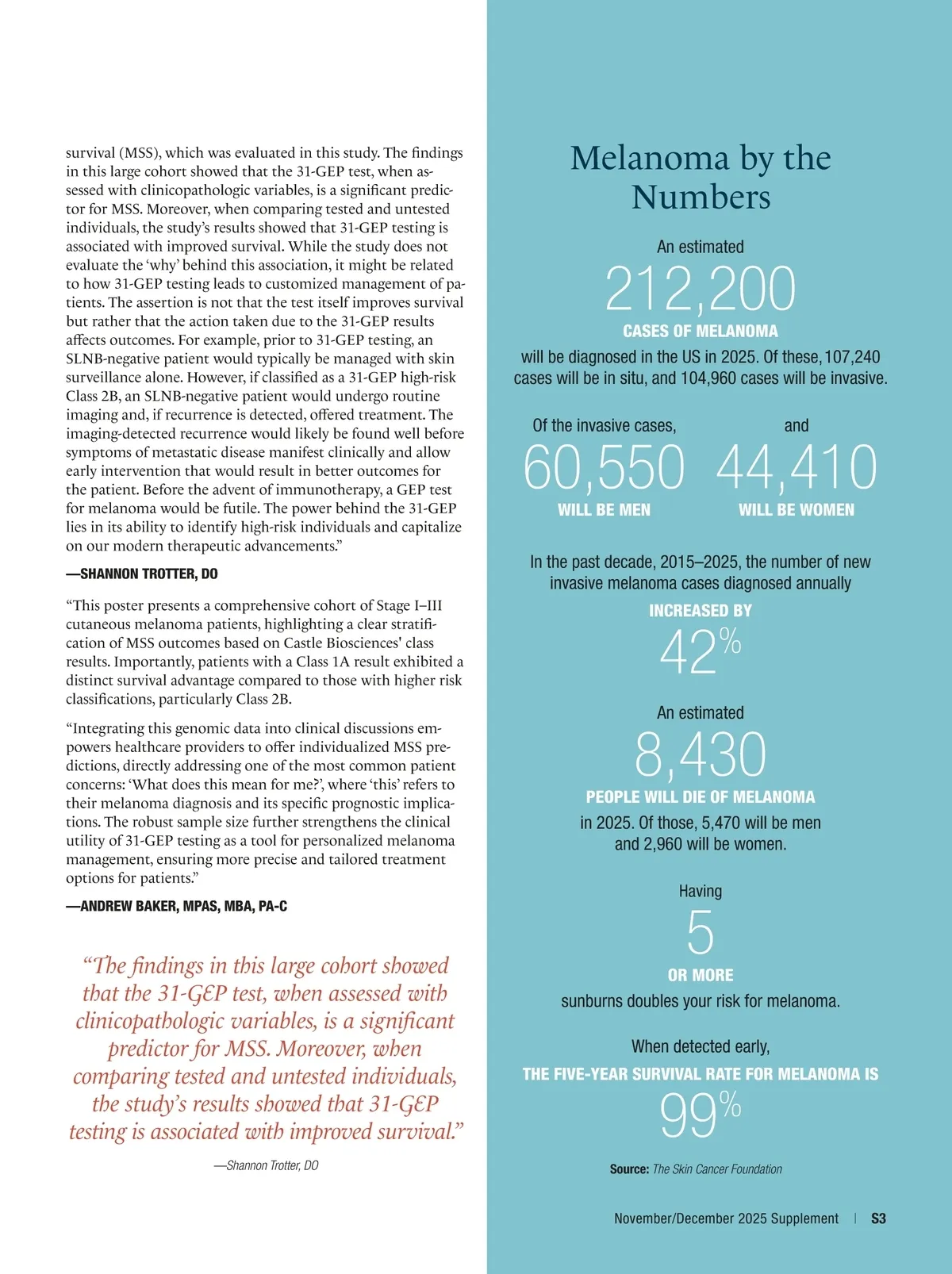
doctors think that a different primary tumor was the source of his metastases. His experience, however, reinforced the seriousness of any melanoma diagnosis and made me an even stronger advocate for encouraging all patients to have the DecisionDx-Melanoma test done when it is offered. Although the prognosis is excellent for the vast majority of ear-ly-stage melanomas, lifetime cure is not guaranteed. I know from my dad’s jour-ney that some early-stage tumors can be highly aggressive. The DecisionDx-Melanoma test provides additional information that can help identify those situations and allow patients and their physicians to make the best possible decisions about their care. MELANOMA About 212,200 cases of melanoma will be diagnosed in the United States in 2025, and an estimated 8,430 people will die from this cancer in the same year, accord-ing to the Skin Cancer Foundation. DecisionDx-Melanoma helps guide decisions regarding sentinel lymph node biopsy (SLNB) for melanoma patients. 212,200 NEW MELANOMAS WILL BE DIAGNOSED IN THE UNITED STATES IN 2025 About Hasanov M, Martin B, Morgan-Linnell SK, et al. The 31-gene expression profile can guide better risk-aligned care decisions for patients with stage I-III cutaneous melanoma: an NCI-SEER analysis. POSTER PRESENTED AT: The 2025 Annual Meeting of the American Society of Clinical Oncology; May 30-June 3, 2025; Chicago, IL. Accessed September 10, 2025. https://www.asco.org/abstracts-presentations/ABSTR ACT495710 Several prospective studies have shown that the 31-gene expression profile (31-GEP) for Stage I–III cutaneous melanoma provides a more personalized estimate of risk for likelihood of sentinel lymph node positivity, recurrence, and mortality than American Joint Commit-tee on Cancer (AJCC) staging alone. This study involving a large, real-world cohort of patients demonstrated the ability of the 31-GEP to identify patients at high-est risk of melanoma-specific mortality within AJCC sub-stage groups. The research was done by linking data from the National Cancer Institute’s (NCI) Surveillance, Epidemiology and End Results (SEER) Program for patients with stage I–III cutaneous melanoma (2013–2019) to data from Castle Biosci-ences for 13,560 patients with 31-GEP re-sults. Within each AJCC sub-stage group (I–IIA, IIB–IIC, III), Kaplan–Meier analy-sis with log-rank test revealed significant differences in five-year melanoma-specific survival rates comparing patients with a Class 1A 31-GEP result vs. those with a Class 1B/2A and Class 2B result ( P < .001 for all sub-stage groups). A multivariable analysis confirmed that the 31-GEP is a significant predictor of melanoma-specific mortality. Results of an analysis comparing 31-GEP tested and untested patients matched based on clinicopathological factors, diagnosis year, ethnicity, and socioeconomic status showed the tested cohort had a statis-tically significant ( P < .001) 32% lower mortality rate. “This study looks at the 31-GEP test in a real-world large cohort of patients and breaks down risk within each AJCC sub-stage group. This stratification is helpful to show outliers designated as high risk by 31-GEP (i.e., Class 2B) in each stage, including Stage IA, Stage IB, and Stage III patients. A possible clinical application extending from this finding might be using the 31-GEP test as a part of decision-making for Stage IIB and IIC patients when considering pembrolizumab (Keytruda, Merck). In addition, it reinforces the ability of the 31-GEP test to identify low-risk (i.e., Class 1A) patients in these stages, which is particularly meaningful in the Stage III group because the 31-GEP test can inform discussions on systemic therapy. Not all Stage III patients have aggressive disease, and so a low-risk 31-GEP result for a Stage III patient might support the decision for that individual to not receive systemic therapy, especially if there are concerns about the patient’s health status and potential morbidity associated with treatment. “The gold standard for a test or ther-apeutic in oncology is its impact on overall survival. From my discussion with multiple colleagues, dermatologists often focus more on melanoma-specific S2
The Dermatology Digest November/December 2025 Castle Supplement: S-2